
Objective
To evaluate the efficacy of twice-daily alcohol-containing, essential oil mouthrinse (LISTERINE® Antiseptic) and brushing, and flossing and brushing, under once-daily supervision for the prevention and reduction of plaque and gingivitis.*
*Floss is intended to remove plaque and food particles between teeth to reduce tooth decay.2
Methodology
Primary endpoints were interproximal mean Modified Gingival Index (MGI) and interproximal mean Turesky Modification of the Quigley-Hein Plaque Index (TPI) at Week 12. Interproximal mean bleeding index (Bl) at Week 12 was a secondary endpoint.
All subjects were supervised once daily at the clinic, Monday through Friday. Second treatment of the day, Saturdays, and Sundays at home were unsupervised and recorded in diaries
For all oral examinations, subjects refrained from oral hygiene for 8-18 hours and did not eat for ≥4 hours before the visit
SUBJECTS (N=156) WERE RANDOMIZED INTO 4 GROUPS:
Inclusion criteria: aged ≥18 years; good general and oral health; no known allergies to commercial dental products; ≥20 teeth with scorable facial and lingual surfaces; evidence of gingivitis; ≥10 bleeding sites based on the Bl; and absence of: fixed or removable orthodontic appliance or removable partial dentures, significant oral soft tissue pathology excluding plaque-induced gingivitis, and advanced periodontitis based on a clinical examination and discretion of the investigator/dental examiner.
Exclusion criteria: dental prophylaxis within 1 month prior to the Baseline visit; need for antibiotics prior to dental treatment; use of antibiotics, anti-inflammatory or anticoagulant therapy within 1 month prior to Baseline; use of oral care products containing chemotherapeutic anti-plaque/anti-gingivitis products within 2 weeks prior to Baseline; use of smokeless tobacco; and any other medical or psychiatric condition that would make the volunteer inappropriate for the study in the judgment of the Investigator.


Results
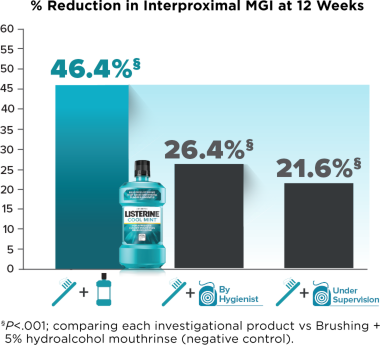
At Week 12, compared with brushing + negative-control mouthrinse, only brushing + LISTERINE® Antiseptic provided statistically significant plaque reduction; and brushing + LISTERINE® Antiseptic, brushing + flossing by hygienist, and brushing + flossing under supervision groups provided statistically significant gingivitis and bleeding reduction.
Compared with brushing + negative-control mouthrinse, interproximal and whole mouth plaque were significantly reduced for the brushing + LISTERINE® Antiseptic group, but not for the brushing + flossing by hygienist or brushing + flossing under supervision groups, at Week 12
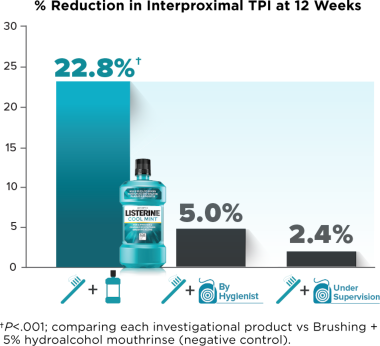
LISTERINE® Antiseptic Significantly Reduced Plaque and Gingivitis:

‡Flossing by dental hygienist. Sustained plaque reduction after a dental prophylaxis.
NOTE: Flossing effectively removes imbedded food particles and biofilm between the teeth, helping improve the health of patients' gums and offering a useful tool in daily oral hygiene. Together, flossing, brushing, and rinsing with LISTERINE® Antiseptic on a daily basis provides a comprehensive approach to oral care and an approach to cleaning that reaches nearly 100% of the mouth.2,3
Compared with Brushing + negative-control mouthrinse, interproximal and whole-mouth gingivitis were significantly reduced for the Brushing + LISTERINE® Antiseptic group, as well as for the Brushing + Flossing by Hygienist and Brushing + Flossing Under Supervision groups
Compared with Brushing + negative-control mouth rise, interproximal bleeding index was significantly reduced in the Brushing + LISTERINE® Antiseptic, Brushing + Flossing by Hygienist, and Brushing + Flossing Under Supervision groups
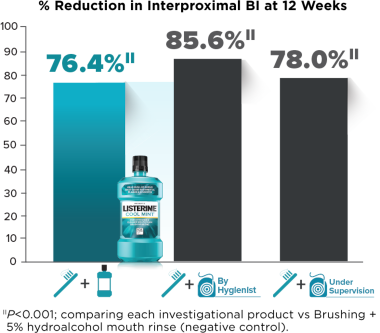
To measure bleeding index, a periodontal probe with a 0.5 mm tip was inserted into the gingival crevice and swept about the tooth at approximately a 60-degree angle. Each of four gingival areas (disto-buccal, mid-buccal, mid-lingual, mesio-lingual) was assessed after about 30 seconds. (0=no bleeding; 1 = bleeding after 30 seconds; 2=immediate bleeding.)
Conclusions
LISTERINE® Antiseptic yielded larger reductions compared to brushing alone in plaque (TPI) and gingivitis (MGI) than hygienist-performed or hygienist-supervised flossing at Week 12
LISTERINE® Antiseptic, hygienist-performed flossing, and hygienist-supervised flossing all statistically significantly reduced interproximal bleeding at Week 12 compared to negative-control mouthrinse
Adding LISTERINE® Antiseptic to an oral care routine reduced supragingival plaque more effectively than flossing by a dental hygienist
Dental professionals may use these data to recommend the most effective oral care routines to their patients depending on their needs
References:
1. Bosma, M.L., McGuire, J.A., Sunkara, A., Sullivan, P., Yoder, A., Milleman, J., Milleman, K. Efficacy of Flossing and Mouthrinsing Regiments on Plaque and Gingivitis: A Randomized Clinical Trial. J Dent Hyg. 2022 Ju 8-20.
2. Floss/interdental cleaners. ADA website, https://www.ada.org/resources/research/science-and-research-institute/or... Last reviewed: September 21, 2021. Accessed February 23, 2022.
3. Kerr WJS, Kelly J, Geddes DAM. The areas of various surfaces in the human mouth from nine years to adulthood. J Dent Res. 1991;70:1528-1530.
Read the editorial "From Research to Practice" in Journal of Dental Hygiene, June 2022: